

| John2290 said: It's in the first ten minutes, the rest is just updates and bullet points for the day. The good Nazi doctor just grabs summeries and sometimes provides commentary from the perspective of both a nurse and a doctor. |
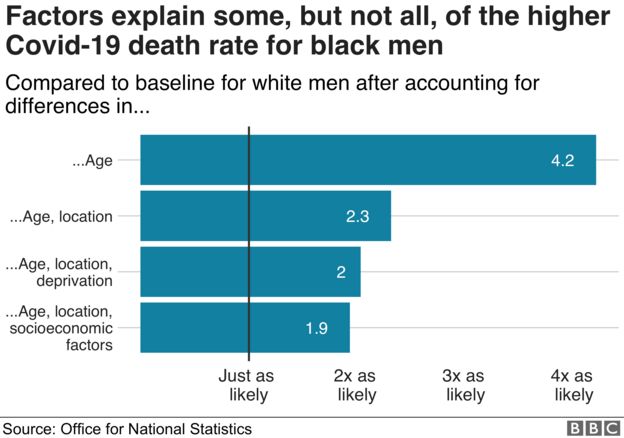
With the limited role Vitamin D seems to play, and the much bigger effect off socio economic status, low income neighborhoods getting hit much harder, it seems the correlation is more linked to income than vitamins.
The USA has data by race as well
https://www.apmresearchlab.org/covid/deaths-by-race
However you need to put it into context of how the virus is spreading through the population:
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial-ethnic-minorities.html
No surprises there, minorities always get the short end of the stick when stuff goes bad.
Where We Live, Learn,
Work, and Play Affects Our Health
The conditions in which people live, learn, work, and play contribute to their health. These conditions, over time, lead to different levels of health risks, needs, and outcomes among some people in certain racial and ethnic minority groups.